By Divya Bhardwaj
By Divya Bhardwaj
The lived experiences of COVID-19 over the past 18-months have exhibited its many socio-economic implications. With governments oscillating between instituting travel bans and lockdowns while fighting recurring waves of COVID-19 cases–lives and livelihoods across the world continue to be gravely impacted.
Months into this pandemic, we observed an increased articulation of constant stress and anxiety due to a sudden loss of control over sustenance, life and future. Vihara conducted longitudinal, design-led qualitative research studies, with remote and in-person data collection in India, specifically in Bihar, Uttar Pradesh, Delhi, and Maharashtra. These studies were conducted with women, men, adolescent girls and frontline workers. The research unpacked COVID-19’s impact on lived experiences, mental stressors, coping mechanisms, as well as potential interventions to address these concerns.
The Second Wave Amplifying the Severity of our Challenge
Our research reveals that what may have been a ubiquitous problem of stress and anxiety, has now led to a pervasive sense of loss, severe grief and trauma, especially since India’s second wave in April-June 2021. In this wave, many experienced the trauma of witnessing near-death experiences themselves or of a loved one, in a time of acute scarcity and an unequivocal breakdown of the health system. Much worse is the guilt, grief and trauma of families who have experienced the loss of one/both parents, a partner, provider or a loved one, with the inability to offer last rites respectfully. Coping with such severe mental health conditions is foremost about acknowledging them, finding support or an appropriate release, and learning to live through it without suppressing the emotions. This could not be further from the reality for women like Radha*, in rural Darbhanga, Bihar, who lost her partner, the provider to her family to COVID-19. With the sudden loss of her husband to an unknown fever with no local doctors willing to touch, let alone cure him – her grief and despair are unparalleled. There is a strong sense of abandonment from both her deceased husband and the system, but what takes precedence is the fear and uncertainty about life and sustenance of her three children. Radha finds odd jobs to put food on the table, with little time to mourn or focus on coping with everything she is feeling. Much like Radha, women in rural India don’t have the privilege to take time off to acknowledge or process their mental health as household and child care responsibilities are solely theirs.
With the added burden of providing for their families due to the dire economic stress that many women face today – there is little opportunity to heal. Vihara’s research also brought to fore the discomfort women feel when pushed into a provider role as it conflicts with their gender role of a caregiver and hinders their capability to perform it.
Correspondingly, our research identified that men experience a constant internal conflict as they are unable to fulfill their gender roles of provider and protector of their families, due to the loss of subsistence or loved ones during this economic and health crisis. Men’s discomfort around acknowledgement and expression of their emotions more often manifests in anger leading to violence and increased dependence on substance abuse. We find that women and girls are at the receiving end of such maladaptive coping. Women and girls are more likely to turn to passivity, self-imposed isolation, and non-communicative behaviours3 thereby impacting their efficacy and capacity to fulfill their responsibilities. This further results in stigmatisation from the unit and the community creating a vicious cycle that disproportionately impacts their mental health and reinforces gender inequalities.
Reassessing Psychosocial Interventions Design
Diverse experiences of grief and trauma exist across gender, age, economic strata, or occupations. Traditional clinical approaches to mental health are proving to be inadequate to these widespread needs, not just due to systemic and digital access challenges, but also due to deficient colloquial vocabulary and stigma around mental wellbeing, especially in low-income resource constraint communities.
Mental health interventions need to be community-led and sensitive to contextualities that may often be triggers or exacerbate stressors. Vihara is keen to build such interventions that focus on enabling individual coping strategies through cognitive behavioural reflections, techniques to navigate triggers, especially for men, where we also need to de-stigmatise expressions of distress and vulnerability.
Given the challenges of articulation of mental health, gamified and narrative tools can greatly encourage sharing and become a way to build emotional support and collaborative familial or couple dynamics. There is a lack of direct channels to adolescents, especially with schools shut and curtailed peer networks. We, therefore, need to leverage available entry points and influencers to provide support and develop escalation pathways where necessary. Interventions that focus on adolescents need to also focus on skill-building, both commercial and life skills, to navigate the social stressors impacting their mental wellbeing.
In addition, the sharp increase in access to mobile internet for women in India is an opportunity for digital innovations if designed with a focus on contextual and behavioural insights. In urban and peri-urban areas, digital solutions must be envisioned to normalize a dialogue around mental wellbeing, equip communities to recognise the symptoms of poor mental health and ways to build healthy active coping behaviours by providing sustained support without fear of judgement.
The COVID-19 pandemic has amplified the need for mental wellbeing interventions that equip men, women, and adolescents to navigate various stressors within and outside of homes. Vihara is committed to designing interventions that consider regional variance around digital access-literacy to develop in tailored offline-online models that are more culturally embedded, contextually rooted and are built on human-centred design approaches for them to be effective and transformative in a meaningful way.
About the author:
Divya Bhardwaj leads the work in gender, social vulnerability, and psychosocial health at Vihara Innovation Network. She brings expertise on social and environmental factors that perpetuate vulnerability, and their impact on behaviours, mental models and decision-making patterns. She directs human-centred design and research projects in RMNCH+A, Covid-19, and has worked across India and Kenya.
Vihara Innovation Network is an impact and innovation firm that uses anthropological research, human-centred design and systems thinking to unpack barriers and design interventions that are inclusive and equitable. We have been working in the development sector for the past 17 years across Asia and Africa.

 By Nivedita Narain, Soledad Artiz Prillaman, and Natalya Rahman
By Nivedita Narain, Soledad Artiz Prillaman, and Natalya Rahman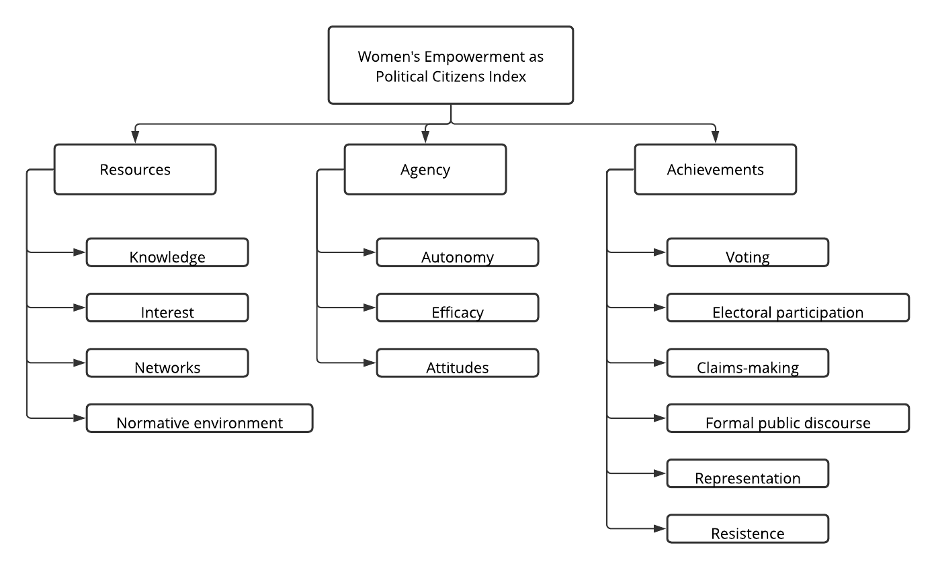 Figure 1: Conceptual framework for political empowerment
Figure 1: Conceptual framework for political empowerment